Pilates has been praised for its ability to strengthen the core and improve posture, but we don’t often talk about the limitations of Pilates. We exist to move and, in daily life, we’re often bending, stretching, twisting and reaching. In technical terms we can say that we are moving through planes of movement around an axis.
|
Plane
Sagittal Anterior-posterior |
Axis
Coronal Frontal, Lateral |
Description
Bisects the body from front to back, dividing it into left and right halves. Flexion and Extension movements usually occur in this plane, i.e. front to back movements |
| Coronal
Frontal Lateral |
Sagittal or Anterior-posterior | Bisects the body laterally from side to side, dividing it into front and back halves. Adbuction and Adduction movements occur in this plane. |
| Transverse Horizontal | Vertical | Divides the body horizontally into Superior and Inferior halves. Rotational movements usually occur in this plane. |
Many functional activities consist of movement in multiple joints, in all 3 planes e.g. getting out of a car consists of hip and trunk flexion (sagittal), hip abduction (frontal) and trunk rotation (transverse)
However, if we look at the strict 34 pilates mathwork exercise positions, many of them only work in one plane – often the sagittal. This is all well and good if we have strength deficits into flexion and extension, but the problem is that we don’t just function moving forwards and backwards. Additionally, if we only strengthen into these planes, we start to exclude other muscles that may function better in different directions. For example, I can work on my hip flexors and extensors to strengthen around the hip; but the hip abductors and rotators have a massive effect on hip stability. If I just concentrate on the muscles that work in the saggital plane, to the exclusion of all others, I am not maximising my body’s movement/strength capability. This uni-planar focus can start to create muscle imbalances which may eventually contribute to injury. Out of the 34 classical positions there are only 4 tri-planer exercises, and 8 bi-planer
But how do we remedy this?
Start by thinking about how we move in daily life. We lunge and twist to pick something off the floor. Even getting out of bed requires movement in all planes. It may be of benefit to modify the standard pilates exercises to include multiplanar movements which mimic function and are more transferrable to daily life. If we want to improve our ability to walk upstairs then that type of movement is what we need to practice. So, in this example, you may get a client to do a lunge (twisting towards the front leg) and come up into a single leg balance as they bring the back knee forward and twist towards the lifted leg. This exercise mimics the movement you need for stair climbing i.e. hip and knee flexion into extension with trunk rotation. All the while still thinking about our core pilates principles namely Centring, Control, Concentration, Breathing, Precision and Flow.
Perhaps we need to think more about what our clients need to accomplish in daily life in choosing our exercises. Specific core activation is great and very much needed in many cases, but we can’t stop there. We need to progress movements by making them more functional and this often helps the client link what they do in the pilates room with what they do outside. There’s more of a carryover into work and sport if they can see how the exercises relate to what they do with their time. So I’m not suggesting we completely forget about the core 34, but I do recommend that we start to think about how we can tweak these exercises, or add new ones, to meet the specific needs of our clients. The body is built to move in various directions so let’s make sure our treatment plans reflect that.
i.e
| Exercise – Main Phase Flow Sets | Objective | Video Link |
| Plank Strength Series
1. Slow push up to plank set up 2. Side plank to hip rotator R 3. Plank set up to slow push up 4. Side plank to hip rotator L 5. Pike Release 6. Toe plank set up 7. Slow toe push up to shoulder tap L 8. Slow toe push up to shoulder tap R 9. Pike Release |
Large supine strength set using core and upper body. Working through sagittal plan into transverse plane at shoulder and spine
|
|
| Swim Flow Series
1. Swan Dive to Swim 2. Swim to sky diver lift 3. Scorpion lift L & R 4. Childs pose release 5. Repeat 1-3 |
Extensor chain strength set working through the opposing sagittal plane with transverse plane introduced to open up frontal spiral line | |
| Side Lying Kick Series
1. Side lying torpedo position to 2. Side lying kick to 3. Side plank set up to 4. Side bend kiss to 5. Side kneeling kick 5 pulses each way to 6. Side kneeling single leg circles 5 each way 7. Plank set up 8. Plank thread the needle to side plank chest opener each side Repeat to opposite side |
Frontal plane lateral line strengtheners introducing transverse plane movement to open up back superficial lines/cross slings through to front spiral lines |
Neurological Wind-up
All the nerves in the body form a continuous network. So the nerves supplying your face are (via the spinal cord) connected to the nerves supplying your toes! This means that irritation in one area of the nervous system can cause problems elsewhere because of how the nervous system is connected e.g. nerve irritation in the lower back can cause symptoms to refer to the buttock/back of thigh/leg via the sciatic nerve which traverses the back of the thigh. But what causes this irritation of the nerves
There are various things which can contribute towards this irritation, but a big factor is lack of movement. The nerves of the body are surrounded by muscle and connective tissue as they travel towards their destinations, and they need to be able to slide between these tissues to function optimally. We call this sliding movement neurodynamics. If the surrounding tissue/muscle is stiff/tight and not allowing that sliding movement; the nerve doesn’t move as freely through the surrounding structures. This leads to tethering and nerve irritation which can cause pain anywhere along the distribution of that nerve.
As nerves supply muscle, any muscle that the nerve supplies will also be affected. Irritation can cause a nerve to become more active. Increased firing of action potentials then increases the activity of the muscles supplied by that nerve and you get what we call increased resting tone i.e. the muscles get tighter. Increased activity of nerves = increased activity/contraction of muscle = tight muscles = further reduced sliding capability of the nerve. This starts to create a vicious cycle of nerve irritation, muscle tightness, reduced nerve sliding and more irritation. Which, in turn, leads to a general stiffening up of parts of or all of the body as movement is reduced. But how do we combat this wind-up?
By releasing the tight muscles and connective tissue surrounding the nerve we can start to improve the nerve sliding ability. Foam rolling is a great way to release tight connective tissue and, as nerves are completely surrounded by connective tissue, reducing that tightness can often have an immediate effect on restoring neurodynamics. Rolling will also have an effect on releasing tight muscles that may be compressing a nerve. Other ways to release tight muscle include stretching and hands on soft tissue release.
Nerves also just enjoy movement as this helps them ‘slide’ between tissues. Interestingly enough, they don’t respond too well to tension so stretching nerves tends to irritate them. There are specific nerve gliding exercises that you can do to target specific nerves, but large range movements also work well to target the neural system as a whole. Some great pilates moves that will accomplish this include standing Roll downs, the Rollover and the Saw. These moves facilitate widespread sliding of nerves and connective tissue, as well as mobilisation of the entire neural network. If the nerves are moving well, they won’t fire as much which will reduce the resting tone of muscles and allow freer movement that is unlimited by tissue tightness.
Myofascial line
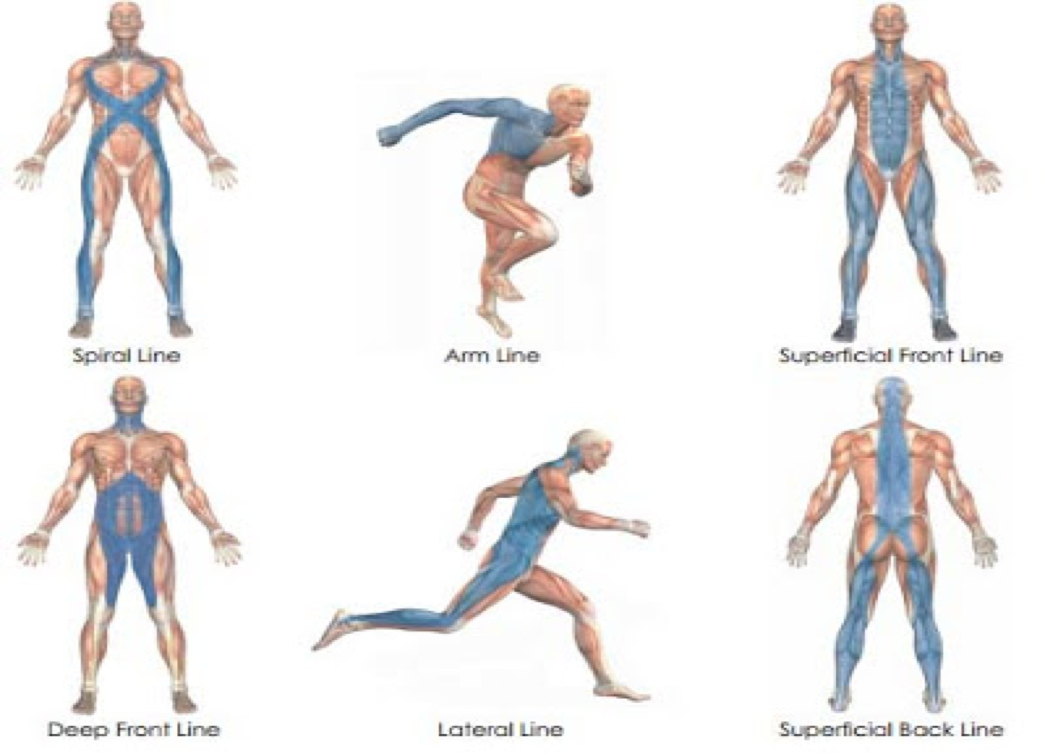
We’re taught that the musculoskeletal system is made up of various muscles (and bones). We then separate those muscles and label them according to where they are (origin and insertion), what they do (action) and how they work (nerve supply). So quadriceps extend the knee and that’s it right? But in reality muscles don’t exist in isolation. Every muscle is connected to its surrounding muscles/structures via connective tissue or fascia. This means that you can follow a myofascial line all the way from the sole of your foot to the top of your head (myo = muscle, so muscle + fasica = myofascial). The view of the body as a sum of individual parts is falling out of favour in the anatomical world. Now professionals are looking more at how everything in the body is connected and how nothing can be viewed in isolation. This has led to the development of the concept of myofascial lines which consist of a series of muscles connected by fascia. These muscles often work together functionally to produce and transmit force throughout the body. Forces move along the line from muscle to muscle, which means that tension at one end of the myofascial line can cause tension along any of the other muscles in that same line. Thomas Myers has described 12 myofascial lines. Following are a few examples:
- Superficial Front Line
Extensor Digitorum Longus and Brevis
Tibialis Anterior
Patellar Tendon
Quadriceps (including the Rectus Femoris)
Rectus Abdominis
Sternalis
Sternocleidomastoid
- Superfical Back Line
Flexor Digitorum Brevis
Gastrocnemius
Hamstrings
Sacrotuberous Ligament
Erector Spinae
Scalp Fasci
- Lateral line
Peroneus Longus and Brevis
Anterior Ligament of the Fibular Head
It-Band, TFL, Glute Max.
Lateral Abdominal
External and Internal intercostals
Splenius Capitis and SCM
- Back Oblique (Functional) Line
Latissimus Dorsi
Posterior layer of the thoraco-lumbar Fascia
Contralateral gluteus maximus
Superficial fascia lata of the ITB (iliotibial band)
Vastus Lateralis
Subpatellar Tendon
This sling system runs at a right angle to the joint plane of the SIJ and in effect will cause closure of the joint when the Latissimus and contralateral gluteus maximus contract.
- Anterior Oblique(Functional) Line
External oblique,
Internal oblique
Transverses Abdominis (TVA) via the rectus sheath,
Contralateral adductor muscles via the adductor-abdominal fascia.
- Spiral line
Anterior View
Splenius capitus
Rhomboids
Serratus anterior
External oblique
Rectus sheath
Internal oblique
Tensor fascia latae
ITB
Tibialis anterior
Posterior View
Peroneus longus
Biceps femoris S/L head
Sacrotuberous ligament
Spinae Erectors
| Posterior Oblique Sling | Anterior Oblique Sling |
|---|---|
 |
 |
So working to release and strengthen these myofascial lines using whole body movement can have a much bigger functional impact than working on specific muscles in isolation. Rather than looking at individual puzzle pieces and trying to make sense of them; we look at how all the pieces fit together to create a bigger picture. Consider with your Pilates exercises adding movement and flow to the uni planar or bi planar positions.
If you would like to know more about this topic, join us on our Pilates Diploma Long Course our Postural Analysis and Movement Correction module or our unique Therapy Exercise Courses